Six Tick Misconceptions 07/05/2012
Posted by thetickthatbitme in Diagnosis, Prevention, TBI Facts.Tags: Babesia, Borrelia, Colorado Tick Fever, health, Lyme Disease, medicine, misconception, Ornithodoros, prevention, Rickettsiosis, Rocky Mountain Spotted Fever, tick, Tick-borne disease
4 comments
I have a confession to make. I have a phobia of most creepy-crawly things–roaches, mosquitoes, spiders, and especially ticks. When I see pictures of any of these critters, my first instinct is to shield my eyes. Ick! But what I should be doing is taking notice, so that if a tick ever gets on me again, maybe I can identify that little jerk.

This tick I can stand to look at. (Image via templeofcartoonmojo.blogspot.com)
Today’s post is about the misconceptions that many people have about ticks. As I warn frequently, there’s a lot of misinformation about ticks and the diseases they spread in the mainstream media and on the Internet. Here are six big misconceptions.
#1: Only deer ticks transmit diseases.
Deer ticks (a.k.a. blacklegged ticks) carry a lot of pathogens, including those that cause Lyme disease, Anaplasmosis, Babesiosis, and Bartonellosis, but they’re not the only ones you need to worry about. Dog ticks (Dermacentor variabilis) and wood ticks (Dermacentor andersoni) carry Rocky Mountain spotted fever (Rickettsiosis), Tularemia, and the Colorado Tick Fever virus. The lone star tick (Ambylomma americanum) carries Ehrlichiosis and the pathogen that causes STARI; bites from this tick have also been linked to a delayed allergic reaction to red meat. Two other types of Rickettsiosis, Rickettsia parkeri and 364D Rickettsiosis can be transmitted by the Gulf Coast tick (Amblyomma maculatum) and the Pacific Coast tick (Dermacentor occidentalis), respectively. Q fever (Coxiella burnetii) can be transmitted by the brown dog tick (Rhipicephalus sanguineus), Rocky Mountain wood tick (Dermacentor andersoni), and the lone star tick (Amblyomma americanum). Last but not least, soft-bodied ticks like Ornithodoros hermsi, Ornithodoros parkeri, and Ornithodoros turicata transmit Relapsing Fever-causing species of Borrelia. These ticks can live up to ten years!
#2: Lyme disease is the most dangerous thing I can get from a tick.
Though life-threatening complications like myocarditis can occur in the later stages of Lyme disease, B. burgdorferi infection is rarely fatal in the first months of infection. Many patients survive years without being properly diagnosed and treated. By contrast, Rickettsiosis (Rocky Mountain spotted fever) can be fatal in the first 8 days of symptoms (which vary greatly from person to person and don’t always involve the spotted rash) if it goes untreated. Female tick saliva also contains a neurotoxin that can cause tick paralysis, which can be fatal if the tick is not found and removed.
#3: I can’t get sick unless the tick is attached 36-48 hours.
While the CDC claims this is true for Lyme disease, if the tick has bitten you, there’s always a chance that bacteria or a virus is already in your system. Even if the tick doesn’t infect you with bacteria or a virus, you are still at risk for tick paralysis (see #2). In the case of soft-bodied Ornithodoros ticks, which spread Relapsing Fever Borrelia, feeding may only take a few minutes, and then the tick falls off, often undetected. (You can read more about soft-bodied ticks here.)
#4: If I don’t go hiking or camping, I’m not going to get bitten by a tick.
While participation in these activities does put you at higher risk for tick exposure, ticks can hide out in plenty of other places besides the forest floor, including the leaf litter in your yard. Ticks can hitch a ride into your yard on any of the wildlife on which they feed, including deer, mice, squirrels, and birds. They can hitch a ride into your house on your dog or cat. And don’t forget other four-legged friends like horses and sheep. If you have mice in your house or attic, you probably also have ticks. To avoid exposure, you should limit your contact with leaf litter, tall grasses, wood piles, and bird feeders. When hiking, stay in the middle of trails, wear long pants tucked into your socks, and wear repellent. Avoid sleeping in cabins that may be infested with rodents (and thereby ticks). After spending time outdoors or with animals, do a thorough tick-check. (This requires getting naked.) And if you’re a fan of spelunking, know that ticks—particularly soft-bodied ones—can live in caves too.
#5: If I don’t have a rash or a fever, the tick that bit me didn’t give me a disease.
At least 20% of people infected with Borrelia burgdorferi (Lyme) don’t have the characteristic erythema chronicum migrans (bull’s-eye) rash (EM). People with other tick-borne illnesses may be asymptomatic or have other symptoms (like joint and muscle pain or fatigue) that may not directly suggest an infection. That’s why it’s important to keep track of all of your symptoms following a tick bite, and to save the tick for identification and testing. You should always make sure your doctor is aware of any tick bites or tick exposures you may have had—and be clear about what regions/countries you’ve visited and what animal exposure you’ve had.
#6: I can use soap or Vaseline to remove a tick, and afterwards I should burn it with a match.
The proper way to remove a tick is with tweezers, grabbing the tick close to the skin, and using a slow, steady motion to pull it out. Using soap or Vaseline will not help you get a better grip on the tick, and may increase the likelihood that you squeeze the tick, causing it to regurgitate bacteria and other pathogens into your skin. Once you remove the tick, you should store it in a secure container and bring it to your doctor’s office for identification and testing. If you do get sick, it will be helpful to know what kind of tick it is and what pathogens it’s carrying. Don’t destroy the evidence with a match! If for some reason you can’t save the tick (because you’re too busy spelunking), at the very least try to take a picture of it. You’ll probably need a zoom lens.
So how do I spot them?
I usually try to link to pictures of ticks instead of posting them on this site because seeing tick photos can be a bit traumatizing to those of us who have been sick with tick-borne infections. However, for the purpose of prevention education, I’ve included pictures of all the ticks mentioned in this post (that I could find) in the slideshow below. You can read about the geographic distribution of hard-bodied ticks in the U.S. here and the habitats of soft-bodied ticks here.
Related articles
Major Misnomer: 8 things you need to know about Rocky Mountain spotted fever 06/05/2012
Posted by thetickthatbitme in Diagnosis, TBI Facts, Treatment.Tags: Arizona, CDC, coinfection, dogs, doxycycline, fatality, Lyme Disease, medicine, rash, Rickettsia, Rocky Mountain Spotted Fever, tick, transfusion
3 comments
The fact sheet for Rocky Mountain spotted fever (Rickettsia) is up today. Here’s the cliff notes version:
1. You don’t have to be in the Rocky Mountains to catch RMSF. There are four types of ticks in the U.S. that can transmit this bacteria to you: the American dog tick (Dermacentor variabilis), Rocky Mountain wood tick (Dermacentor andersoni), brown dog tick (Rhipicephalus sanguineus), and the Cayenne tick (Amblyomma cajennense). Cases of RMSF have been reported all over the U.S., and there have also been some in Canada. In 2008, all but 8 states reported cases of RMSF to the CDC.
2. Rocky Mountain spotted fever can be a deadly disease if not treated promptly. The national fatality rate is about 3%, but this rate is much higher in certain states like Arizona, where the fatality rate is 10%. This is likely due to delayed diagnosis.
3. Patients infected with the Rickettsia rickettsii bacteria that causes RMSF may experience any combination of the following symptoms: chills, confusion, fever, headache, muscle pain, rash, diarrhea, light sensitivity, hallucinations, loss of appetite, nausea, thirst, and vomiting. Though 90% of patients develop the spotted rash, this often comes late in the illness, so if other symptoms are present, you shouldn’t wait to get treated. Ten percent of patients never develop the rash.

Example of an early-stage rash in an RMSF patient. (Image via CDC.gov)
4. RMSF can be diagnosed with a blood antibody test called an IFA (indirect immunofluorescence assay), but this test is often negative in the first week or so of infection. If you are showing symptoms of RMSF, your doctor shouldn’t wait for blood test results before putting you on antibiotics, because the longer treatment is delayed, the higher the risk of fatality.
5. RMSF is treated with Doxycycline in both adults and children. The usual course is between 7 and 14 days. The CDC recommends treating for at least 3 days after fever subsides.
6. Another way to get RMSF is by squashing ticks that you find on your dog (or anywhere else) with your bare fingers. When you squish a tick, the bacteria inside it can come out and enter your body through your skin. When checking your pets for ticks, always wear gloves, and use tweezers for tick removal.
7. Although very rare, it is possible to get RMSF from a blood transfusion. If you experience symptoms of RMSF following a transfusion, see your doctor right away.
8. The symptoms of RMSF can mimic those of other TBIDs, like Ehrlichiosis and Anaplasmosis. Luckily, all three of these are treated with Doxycycline.
If you want to read more about RMSF, check out the fact sheet, which is full of links to additional information.
Related articles
Arthralgias, myalgias, and herx—oh my! (Symptom vocabulary for TBIDs) 05/22/2012
Posted by thetickthatbitme in TBI Facts, Tick-Lit, Treatment.Tags: antibiotics, arthralgia, Bell's palsy, Borrelia, herx, Herxheimer reaction, Lyme Disease, medicine, myalgia, pulse, supplements, tachycardia
add a comment

Oh no, not a Borrelia infection!
This is part one in a multi-part series on vocabulary related to tick-borne infectious diseases (TBIDs). Today, we focus on symptoms. You can find all these terms and more on the Glossary page.
arthralgia: a fancy medical term for joint pain. The origin is Greek (arthro- = joint; -algos = pain). Arthralgias may be a symptom of injury, infection, illness, or an allergic reaction. They are a common symptom with TBIDs like Borrelia burgdorferi (Lyme Disease), Borrelia hermsii (TBRF), and Babesia.
myalgia: a fancy medical term for muscle aches. Myalgias can be a symptom of infection with Borrelia burgdorferi (Lyme Disease), Borrelia hermsii (TBRF), Babesia, Ehrlichia, Anaplasma phagocytophilum, Rocky Mountain Spotted Fever, Toxoplasmosis, Malaria, or Influenza. They can also be a symptom of inflammatory diseases like Multiple Sclerosis.
Bell’s palsy: This is a paralysis of the muscles in the face caused by damage to the seventh cranial nerve. It is often unilateral (only on one side), and it’s more commonly seen in patients with Borrelia burgdorferi. As you may know, one of the consequences of Borrelia infection is inflammation, and this inflammation can lead to loss of nerve function. You can read more about Bell’s palsy here. Patients with Borrelia infections may also have damage to the eighth cranial nerve (also known as the auditory vestibular nerve), which can result in tinnitus (ringing of the ears) and problems with balance.

A pulse oximeter measures pulse and oxygen. Image via Yale Medical Group.
postural tachycardia: Tachycardia is a heart rate that exceeds the normal range (usually indicated by a pulse greater than 100). Some people with infections have tachycardia all the time, but many only have postural tachycardia, which is tachycardia when you stand up for 3 minutes after lying down for 3 minutes. According to my doctor, this has been a great predictor of whether a patient has an infection, and he puts every new patient though the “tilt test”: lie down three minutes, have your vitals taken, stand up 3 minutes, have your vitals taken. Often, the difference in lying and standing pulse will decrease over the course of treatment.
herx: Herx is short for Herxheimer reaction (or Jarisch-Herxheimer reaction). It was named after dermatologists Adolf Jarisch and Karl Herxheimer in the late nineteenth century, who discovered it while treating Syphilis patients with mercury. (Fun fact: Herxheimer was a colleague of Paul Ehrlich, for whom Ehrlichia is named. They both helped found the University of Frankfurt. Not-so-fun fact: Herxheimer was murdered in 1942 by Nazis at Theresienstadt; he was 81.) A Herxheimer reaction can occur when one is being treated for an infection with antibiotics. It’s thought to be caused by the endotoxins that are released as bacteria start to die off. Herx are characterized by fever, chills, rigor (shaking), hypotension, headache, tachycardia, hyperventilation, vasodilation with flushing, myalgia (muscle pain), and exacerbation of skin lesions.
I’ve discovered a bit of an inconsistency when it comes to information available online and in published research about herx. Almost every Lyme patient blog I’ve ever read mentions herxing. I was herxing bad today, etc. Many patient and doctor organizations related to the treatment of Lyme Disease also discuss herxing. They characterize herxing as common among patients with Borrelia infections and as a sign that antibiotics are working. Herx seems to be used liberally as a term that means any sort of increased discomfort that a patient feels while undergoing antibiotic treatment.
For the sake of comparison, let me tell you how a medical textbook describes the Herxheimer reaction. I’m using as my reference Principles and Practices of Infectious Diseases, seventh edition (borrowed, not bought). I’ll start with the Herxheimer reaction as studied in patients with Borrelia hermsii (TBRF) infections. A herx in hermsii patients is characterized by severe rigors, increase in temperature, and decrease in blood pressure. The onset of reaction occurs within 2 hours of initial therapy and coincides with clearing of spirochetes from the blood. This means that in order to have the reaction you have to have spirochetes in the blood (which would be indicated by a positive blood smear). You’ll also notice that the reaction happens on the first day of treatment.
According to Principles and Practices, herx occur in 30-40% of patients with Borrelia hermsii infections. When a herx does occur, medical attention is necessary because there is a possibility of fatality. Aspirin is sometimes given to lower the fever. A saline infusion can be given to increase blood pressure. If the reaction is very severe, the patient may have to be given steroids. In sum, if you have an acute Borrelia hermsii infection and are treated with antibiotics, there is a chance that you will have a herx reaction the first day of treatment. If you are having a true herx, you will probably need immediate medical attention.
Now, you may remember that I had Borrelia hermsii, and upon reading the above information, I was really curious as to why I never experienced one of these reactions. When I asked my doctor about it, he explained that it was because I had a latent infection. In other words, I did not receive treatment until several years after I was infected. My body had already tried to fight off the bacteria, and had partially succeeded because my infection was no longer acute. This meant I did not have a high load of bacteria in my blood. So even though some days my joint and muscle pain worsened and I felt sick to my stomach, because I didn’t have the shaking, the fever, and the low blood pressure and because the bacteria was hiding in my joints, not in my blood, I never had a herx reaction. Dr. W went on to say that he has treated more than 50 people with B. hermsii infections, and he has never seen a herx in clinic. He has, however, seen some fever-chill reactions when patients with hermsii were being treated with Ceftriaxone. “And those weren’t herx?” I asked. He didn’t believe so; rather, he thought that the fever and chills were because Ceftriaxone wasn’t killing the bacteria quickly enough. When he switched those patients to Ertapenem, a stronger antibiotic, the fever and chills went away, and the patients saw improvement in their conditions.
Now here’s what Principles and Practices has to say about herx in patients with Borrelia burgdorferi (Lyme Disease). The reaction occurs during the first 24 hours of therapy, and consists of high fever, a redder rash, and greater pain. Some vasodilatation may also occur. The Herxheimer reaction occurred in approximately 15% of patients. Only 15 percent! That was shocking to read. There were also no reported deaths from Herxheimer reactions during antibiotic therapy for Lyme Disease.
Clearly, the rate of herx reactions in studies did not match my impression from anecdotal accounts from patients, so I asked Dr. W if he could offer any explanation. His hypothesis was that since most B. burgdorferi (Lyme) patients have latent (long-term) infections and not acute (new) infections, they are probably not having true herx reactions. However, since some doctors prescribe a lot of different supplements to be taken while patients are undergoing antibiotic therapy, perhaps some of the symptoms that patients feel are adverse reactions to the supplements. Because supplements are not subject to the same FDA regulation as pharmaceuticals, the companies that manufacture them are not required to prove their safety or effectiveness. Consequently, very little is known about how these products interact with prescription and over-the-counter medications. To read more about supplements and regulation, go here.
Here’s what I take away from all this:
- Herxheimer reaction is a medical term used to describe a specific set of symptoms in a specific set of patients (those with acute Borrelia infections) which may be life threatening (in the case of very high fever and very low blood pressure), particularly in patients with Borrelia hermsii infections.
- The term “herx” has been adopted by both the LLMD (Lyme-literate medical doctor) community and the Lyme patient community and has evolved into a generic, non-clinical term that means discomfort or worsening of symptoms that occurs multiple times throughout the course of antibiotic treatment.
- Just because a patient is experiencing discomfort does not mean he or she is having a true Herxheimer reaction.
- Contrary to what some doctors say, there is nothing worrisome about a patient who does not have a Herxheimer reaction, as they only occur in 30-40% of B. hermsii patients and 15% of B. burgdorferi patients.
- Some episodes of high fever and chills during antibiotic therapy might mean that the antibiotic is NOT working well enough. Patients sometimes benefit by being switched from Ceftriaxone to Ertapenem.
- Because some patients take a number of supplements in addition to antibiotic therapy and none of these are properly regulated by the FDA and studied in clinical trials, their effect on the body is unpredictable. It’s possible that some reactions that patients believe are Herxheimer reactions are actually reactions to other things they are taking.
Related articles
- My Story (thetickthatbitme.com)
- Ceftriaxone (Rocephin): Is your doctor following directions? (thetickthatbitme.com)
- Curious about Tick-borne Infections? (thetickthatbitme.com)
Stuff I’ve been tested for and WHY 05/08/2012
Posted by thetickthatbitme in Diagnosis, TBI Facts, Whole Person.Tags: Anaplasma phagocytophilum, Babesia, Bartonella, Borrelia, Ehrlichia, food poisoning, health, labs, Lyme Disease, medicine, pets, Quest Diagnostics, ticks
add a comment
I apologize for the inconsistent posting lately; it’s been a busy couple weeks. No tick-lit today, so I’ll owe you some later in the week!
Tonight’s question: How did my doctor find 3 crazy infections that five other doctors missed? (One of which went undiagnosed for 7 years!)

This is the small binder I carry with me to doctor’s appointments. I have about half a file drawer dedicated to the rest.
Answer: He sent me to get tested for a whole lot of stuff.
How did he know what to order? He considered my risk factors and exposure to disease vectors (like ticks and pets). Is it important for your doctor to know if you’ve been out of the country? If you used to live in another state? If you have pets? If you hike or camp? If you’ve had food poisoning? Yes, yes, yes, yes, and yes!
Below, rather than listing the name of each disease/infection I was tested for, I’ve listed the names of the tests as they appear in my lab reports from Quest Diagnostics. (No, Quest did not pay me to mention their name. I just happen to like them, since they’re always nice to me and their tests helped find my infections.) They’re sorted according to why my doctor thought to order them.

Quest sends me pretty labs in color (as if that matters). Tip: always check the box on your lab slip that says “mail patient a copy” or something like that.
DISCLAIMER: Just because I’ve been tested for something doesn’t mean that you need to be. Only you and your doctor can decide what you should be tested for based on your history, risk factors, and symptoms.
Tick exposure
Borrelia hermsii AB IFA
Ehrlichia chaffeensis IFA
Lyme Disease Antibody (IgG/IgM) Western Blot
WA1 (Babesia duncani) IgG Antibody, IFA
Babesia microti Antibody IgG/IgM
Cat exposure
Bartonella Species Antibody test w/reflex (FYI: One of my cats has tested positive for Bartonella, but I was negative. He’s never scratched or bitten me, but I have been bitten by a different cat.)
Toxoplasma IgG Antibody
Toxocara Antibody, ELISA (serum)
Having food poisoning in Mexico and China
Entamoeba histolytica IgG, ELISA
Giardia lamblia AB Panel, IFA
Helicobacter pylori breath test
Salmonella and Shigella Culture (this was not fun, but I’m glad they were negative)
Camphylobacter Culture
Additional tests:
Immunoblobulins G, A, and M (to see if I was deficient, as this would affect the results of antibody tests and would mean I might need additional treatment, like IVIG—luckily I was not deficient)
CBC (to see if I was low on any particular kinds of blood cells, which might indicate an infection)
Questions? Feel free to comment/e-mail. For whatever reason, I seem to enjoy discussing labs.
Ehrlichia: confusing cousins, the blood supply, and the new kid on the block 05/04/2012
Posted by thetickthatbitme in Diagnosis, TBI Facts.Tags: Blood donation, Blood transfusion, CDC, Ehrlichia, health, Lyme Disease, medicine, Minnesota, Rocky Mountain Spotted Fever, tick, Wisconsin
5 comments
Ehrlichia…I just met a girl named Ehrlichia…and suddenly the sound…
Nope. Doesn’t quite work.

Paul Ehrlich (1854-1915). Image via Wikipedia.
Ehrlichia is actually named after German microbiologist Paul Ehrlich (1854-1915), who won the Nobel Prize in 1908. Here are some things you actually need to know about Ehrlichia:
1. Ehrlichia is transmitted through the bites of lonestar ticks and deer ticks. If you’ve had another infection carried by these ticks (like Lyme Disease), your doctor should have had you tested for Ehrlichia (or maybe you’ll be asking him/her to test you after reading this post?).
2. Symptoms of Ehrlichiosis include: fever, headache, chills, malaise, muscle pain, nausea / vomiting / diarrhea, confusion, conjunctival injection (red eyes), and rash (in up to 60% of children, less than 30% of adults). When it goes untreated (or improperly treated), complications can include breathing problems, bleeding disorders, and death (1.8% of cases).
3. Ehrlichia is effectively treated with doxycycline in both adults and children. The CDC recommends a 7-14 day course.
4. Your doctor shouldn’t wait for your test results to come back before prescribing you doxycycline. If your doctor thinks you might have Ehrlichiosis, he/she might order a PCR, a blood smear, or an IFA (antibody test). These tests can take a few weeks to come back, and in that time, you could get very, very sick. In addition, a negative result on any of these three tests does not rule out the possibility of infection. Often, in the first 7-10 days you are infected, you will test negative. For more information about these tests, take a look at the Ehrlichiosis fact sheet.
5. Ehrlichia can be easily misdiagnosed as one of two other infections. It’s a rickettisial disease, which means it’s in the same family with A. phagocytophilum and Rocky Mountain Spotted Fever (RMSF). Sometimes the rash patients get with Ehrlichia looks a lot like the rash patients get with RMSF.
6. It may be possible to contract an Ehrlichia infection through a blood transfusion. The CDC has not been very vocal about it, but it’s on their website. Fun fact: “Ehrlichia chaffeensis has been shown to survive for more than a week in refrigerated blood.” If you’ve had an Ehrlichia infection, it’s probably not a good idea for you to be a blood or organ donor.
7. There’s a newly identified species of Ehrlichia in Wisconsin and Minnesota. It doesn’t have a fancy species name yet, so scientists refer to it as Ehrlichia Wisconsin HM543746 or Ehrlichia muris-like (EML). This one is carried by deer ticks. If you live in one of these states and your doctor is not so hip to the new infectious disease research, he or she may have told you that you didn’t need to be tested for Ehrlichia because “we don’t have that here.” (I hate it when doctors say that!)Hopefully there will be a commercially-available, species-specific test for this soon. For now, my guess is that physicians in Wisconsin and Minnesota who suspect Ehrlichia infection are ordering tests for E. chaffeensis and E. ewingii.
Got an Ehrlichia story you’d like to share? Shoot me an e-mail.
Related articles
Well, Babs, you’re trickier than I thought 05/01/2012
Posted by thetickthatbitme in Diagnosis, Peer-Reviewed, TBI Facts, Tick-Lit.Tags: Babesia, Blood donation, Blood transfusion, health, IFA, labs, Lyme, medicine, PCR, smear, tick
1 comment so far
Welcome to the second installment of Tick-Lit Tuesday, where I comb through PubMed so you don’t have to. Today’s topic: Babesia and Blood Transfusions. Now, I know I posted about Babesia in the blood supply just a few days ago, but an interesting study has since come to my attention (thanks, Dr. W), and the implications are a bit scary. Okay, get your popcorn and let’s begin.
The Issue:

A blood donation pictogram. Image via Wikipedia.
It has been well-documented that the tick-borne protozoan parasite Babesia can be contracted through blood transfusions. Blood centers aren’t required to test donated blood for Babesia, but this may change in the future, as Babesia infections contracted through transfusions are on the rise. So if we were to test all donors for Babesia prior to donation, which tests should we rely on to detect this pesky parasite? Let’s look at the candidates.
IFA: IFA is an abbreviation for indirect fluorescent antibody test. This type of test can also be referred to as serologic (as in blood serum) testing. If you’ve had one of these tests for Babesia, it’s probably titled something like “WA1 IGG ANTIBODY IFA” (for B. duncani) or “BABESIA MICROTI ABS IGG/IGM” on your lab results. If you’ve had Babesia in the past and been treated for it, your antibody test might still read positive because your body is still making antibodies to the parasite. This is one of the reasons why most insurance companies refuse to pay for treatment for Babesia if your only positive test is the IFA. They think maybe you had a past infection that you got over, so you don’t need treatment. (The other reason they refuse to pay is that they’re jerks, to put it nicely.) I’ll talk more about why this is such a problem later in this post.

A stained blood smear on which B. microti parasites are visible in red blood cells. (CDC Photo: DPDx). Via CDC.gov.
Smear: When we talk about a smear for Babesia, we mean a Giemsa-stained thin blood smear. This test involves looking at blood samples under a microscope to see if there are any parasites hanging around. The problem with this test is that Babesia can infect fewer than 1% of your circulating red blood cells, so it could take many, many smears before any Babesia show up under the microscope. For more information about that phenomenon, read this.
PCR: This stands for polymerase chain reaction. It’s basically a DNA test that tries to identify whether a gene associated with Babesia is present in the blood. PCR has been found to be “as sensitive and specific” as blood smears for Babesia (see this study), which is not saying much, considering the tendency of Babesia to go undetected with smears.
Hmmm, for whom shall I cast my ballot, the antibody test insurance companies don’t trust, the inaccurate smear, or the inaccurate PCR? Choices, choices…
Today’s question:
Can the donated blood of someone with a negative PCR and negative blood smear still be infected with Babesia and cause Babesia infection in transfusion recipients?
(Hint: This is a leading question.)
Let’s talk about a study published in the journal Transfusion in December of 2011 called “The third described case of transfusion-transmitted Babesia duncani.”
Here’s what happened:
In May 2008, a 59 year-old California resident (I’ll call him Cal) with sickle-cell disease had some red blood cell transfusions. Cal’s only risk factor for Babesia was the transfusions; he didn’t have any tick exposure. In September of 2008, Cal was diagnosed with a Babesia duncani (WA-1) infection. The parasites were visible on a blood smear, the indirect fluorescent antibody (IFA) test was positive, and the PCR was positive for the Babesia gene. This launched a transfusion investigation in which doctors tracked down 34 of the 38 blood donors whose blood could have infected Cal with Babesia. One donor, a 67-year-old California resident (who I’ll call Don) had a B. duncani titer of 1:4096 (on the IFA test). What does a titer of 1:4096 mean? Well, if the antibody test for B. duncani is negative, the titer will be < 1:256. That means that Don’s antibody test was positive.
What the article abstract doesn’t tell you, which the full article does, is that both Don’s PCR and blood smear were negative for Babesia. How did the researchers prove definitively that Don had Babesia in his blood? They injected the blood into Mongolian gerbils, and were later able to isolate the parasite from the gerbils. Conclusion: Even though Don showed no symptoms of Babesia and both his PCR and smear were negative, his donated blood caused Babesiosis in both Cal and the gerbils.
Here’s why the study’s findings are important:
1. Clearly, blood smears and PCRs are not good indicators of whether someone is infected with Babesia. Why insurance companies think these tests need to be positive before they’ll pay for treatment is a mystery to me. There are probably a lot of people out there who’ve had positive IFAs but negative smear and/or PCR who were then not treated for Babesia because either the doctor, the insurance company, or both said they didn’t have an infection.
2. As far as the blood donation goes, if we don’t start screening out donors with positive Babesia IFAs, we’re going to continue to contaminate the blood supply with Babesia. It should be as simple as that. Been bitten by a tick? No blood donation for you. Positive IFA? No blood donation for you.
DZWSQK6QYS9G
Related articles
Four (surprising) places ticks hang out 04/30/2012
Posted by thetickthatbitme in Media, TBI Facts.Tags: Borrelia, Grizzly Peak, health, Lyme, mice, Permethrin, prevention, tick, Tilden Regional Park, yard
4 comments
Most people think you have to be hiking around in the woods to pick up a tick. In reality, ticks are a lot closer than you think. Here are four (possibly surprising) places where ticks hang out:
1. In your un-mown lawn. Ticks like to hide in vegetation to keep from drying out. Vegetation includes tall grasses, so don’t get lazy on the lawn upkeep!
2. In piles of fallen leaves. Yes, leaves are fun to jump in, and yes, the crunchy sound they make when you walk over them is lovely, but you (or your pet) could also be picking up ticks from leaf litter, so rake ’em up!

Ticks feed on and pick up diseases from mice. Image via tickencounter.org
3. Anywhere mice or other rodents live. This includes wood piles, rock walls, crawl spaces, ground covers, abandoned vehicles, garbage, bushes, and palm trees. Mice also like to eat fallen fruit, so if you have fruit trees, be sure to dispose of any fruit that falls. If you have mice or rats in your home, chances are you have ticks, too. Here’s a more detailed list of mouse hiding places and what you can do to keep them away from your yard and house.
4. On and underneath wooden picnic tables and benches. To me, this is the creepiest one, because I’ve been to countless kids’ birthdays and neighborhood get-togethers in the park, and the last thing on my mind was tick exposure. If you don’t believe me when I say the risk is real, here’s an article abstract for a study conducted by Kerry Padgett and Denise Bonilla from the California Department of Public Health.

Park bench on Grizzly Peak, in the Berkeley Hills. Image via Wikimedia Commons. Credit: nickton.
They collected ticks (some of which tested positive for Borrelia) from various areas in Berkeley’s Tilden Regional Park and found as many on wood surfaces as in leaf litter. If you’re planning on a day in the park, I recommend long pants and repellent with Permethrin.
If you’re spending time outdoors, it’s a good idea to check yourself for ticks as soon as you come inside. The University of Rhode Island’s Tick Encounter Resource Center has a great multimedia tool, the Tick Bite Locator, which suggests common places to check for ticks. They also have images of a variety of disease-carrying ticks (although the soft-bodied ones are missing) at different life stages.
Got a dog and not sure how to check him/her for ticks? WordPress blog After Gadget has a detailed explanation of how to do a thorough tick-check.
Be careful out there, everyone!
Related articles
Parasites in the blood supply, and 7 other things you need to know about Babesia 04/27/2012
Posted by thetickthatbitme in TBI Facts.Tags: Babesia, Blood donation, Blood transfusion, health, Malaria, medicine, Mepron, parasite, pregnancy, Rhode Island Blood Center, tick bite
6 comments
The fact sheet for Babesia is up today. Here are a few (disturbing) highlights:
1. Babesia is a parasite that attacks red blood cells. There are three ways Babesia spreads: 1) Through the bite of the blacklegged tick (or deer tick, Ixodes scapularis—the same tick that carries Lyme/B. burgdorferi); 2) Through blood transfusions with contaminated donated blood; 3) From mother to baby during pregnancy or childbirth.

A nymphal stage Ixodes scapularis tick (approximately the size of a poppy seed) is shown here on the back of a penny. Credit: G. Hickling, University of Tennessee.
2. The tick that carries Babesia is most likely to infect humans when it’s in its nymphal stage. During this stage, the tick is about the size of a poppy seed. (Maybe this is one reason why Babesia cases are on the rise among older people–they probably have trouble spotting ticks that small!)
3. Many people who have a Babesia infection don’t show any symptoms. When they do show symptoms, they can include fever, chills, sweats, headache, body aches, loss of appetite, nausea, and fatigue. Some develop hemolytic anemia, which causes jaundice and dark urine.
4. Babesia can be deadly if it goes untreated. Here are some possible complications: low and unstable blood pressure; altered mental status; severe hemolytic anemia (hemolysis); very low platelet count (thrombocytopenia); disseminated intravascular coagulation (also known as “DIC” or consumptive coagulopathy), which can lead to blood clots and bleeding; and malfunction of vital organs (such as the kidneys, liver, lungs, and heart).
5. There are two main treatment options for Babesia: a combination of Mepron and Zithromax OR a combination of Clindamycin and Quinine. Children and women who are pregnant should probably not be treated with Mepron.To read more about treatment, go to the Babesia fact sheet.
6. Babesia is sometimes confused with Malaria because they look similar under a microscope and can have similar symptoms. To avoid confusion, doctors should order multiple types of tests for Babesia if patients show symptoms. To read more about available tests, see the fact sheet.
-
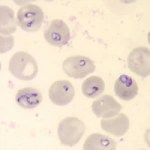
- Babesia parasites in red blood cells on a stained blood smear. (CDC Photo: DPDx). Via CDC.gov.

-
- Blood smear stained with Giemsa, showing a white blood cell (on left side) and several red blood cells, two of which are infected with Plasmodium falciparum (Malaria) (on right side). Image via CDC.gov.

7. There are 4 identified species of Babesia that infect humans: Babesia microti, B. divergens, B. duncani (WA-1), and MO-1 (unnamed strain). Antibody tests for Babesia are species specific, so if you have B. microti and you are tested for B. duncani, the test will come back negative. This means that patients need to undergo multiple blood tests!
8. Even though Babesia infection is known to be transmitted through blood transfusion (As of Sept. 2011, the CDC has identified 159 cases, and at least 12 of those people have died.), donated blood is not tested for Babesia! Donors are asked to fill out a questionnaire asking whether they have Babesia (not whether they’ve had tick bites or Babesia-like symptoms). In other words, we are relying on patient self-reporting to screen the blood supply for this parasite! (Why they don’t screen out all people who’ve had tick bites is beyond me.) The CDC’s response as to whether they will implement testing of donated blood for Babesia in the future: Maybe. They say they are going to “Monitor reports of tick-borne infection to determine if the disease is spreading to other parts of the country and to identify emerging strains of Babesia that may cause human disease.” In other words, they’re going to wait to see how bad it gets before they do anything about the blood supply. Some organizations like the Rhode Island Blood Center have begun screening blood for Babesia using an experimental test, but this is not mandated by CDC policy.
This might prompt you to ask: What are my local health department, hospitals, and blood donation organizations doing about Babesia in the blood supply?
Have questions or something to add about Babesia? Drop me a comment.
Related articles
- Well, Babs, you’re trickier than I thought (thetickthatbitme.com)
Eight things you need to know about Anaplasmosis 04/25/2012
Posted by thetickthatbitme in Diagnosis, TBI Facts.Tags: Anaplasma phagocytophilum, Anaplasmosis, Borrelia burgdorferi, doxycycline, health, labs, Lyme Disease, medicine, Rocky Mountain Spotted Fever, tick, treatment
5 comments
A new fact sheet is up today for Anaplasmosis, otherwise known as Anaplasma phagocytophilum infection. Try saying that three times fast. This is one of the two TBIDs I’ve been unlucky enough to have, but I had never heard of it before my lab results came back with a positive antibody test for it. By the end of this post, you’ll know eight things you didn’t know before about Anaplasmosis.

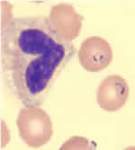
A microcolony of A. phagocytophylum visible in a granulocyte (white blood cell) on a peripheral blood smear. Image via CDC.gov.
1. Anaplasmosis is spread by the same ticks that spread Borrelia burgdorferi (Lyme Disease). This means that people with Lyme can have a coinfection with Anaplasmosis (and some of them don’t know it).
2. The symptoms of an Anaplasma phagocytophilum infection are: fever, headache, muscle pain, malaise, chills, nausea / abdominal pain, cough, and confusion. Some people get all the symptoms; other people only get a few.
3. If you show symptoms of Anaplasmosis, your doctor shouldn’t wait for lab results to come back to begin treating you. The CDC recommends beginning treatment right away.
4. If you’ve been infected with Anaplasma phagocytophilum and you get tested within the first 7-10 days you are sick, the test might come back negative. This doesn’t mean you don’t have Anaplasmosis, and you’ll need to be tested again later.
5. The best way to treat Anaplasmosis is with the antibiotic Doxycycline. According to the CDC, other antibiotics should not be substituted because they increase the risk of fatality. If your doctor insists on treating your Anaplasmosis with something other than Doxycycline, it’s probably time to get a new doctor. For people with severe allergies to Doxycycline or for women who are pregnant, the drug Rifampin can be used to treat Anaplasmosis.
6. Anaplasmosis can be confused with other TBIDs in the rickettsia family like Rocky Mountain Spotted Fever (RMSF) and ehrlichiosis. These infections are also commonly treated with Doxycycline.

Image via CDC.gov.
7. The number of cases of Anaplasmosis reported to the CDC has increased steadily since 1996. You can attribute this to climate change or not, but the trend suggests that this disease will be an increasingly more common problem in the future.
8. More than half of Anaplasmosis cases are reported in the spring and summer months. This is a no-brainer, since this is when tick populations thrive. To avoid infection, take steps to avoid tick exposure for both you and your pets.

Image via CDC.gov.
Curious about Tick-borne Infections? 04/21/2012
Posted by thetickthatbitme in TBI Facts.Tags: Borrelia burgdorferi, Borrelia hermsii, diagnosis, facts, infection, Lyme, Lyme Disease, TBI, tick-borne, treatment, ugly stepsister
2 comments
Happy Saturday, loyal readers!
I thought I’d point out that I’ve added a new section to the blog: Infection Fact Sheets. One of my goals with this blog is to give you, my readers, access to as much factual information about tick-borne infectious diseases–or TBIDs, as I like to abbreviate them–as possible.
Since you’ve stumbled upon this blog, I’m sure you’ve heard of Lyme Disease, but do you know the name of the bacterium that causes it? Are you familiar with the common and not-so-common symptoms? What about the different drugs that are used to treat this infection? Check out the fact sheet here.
And let’s not forget Borrelia hermsii, which I consider to be like Lyme’s neglected ugly stepsister. Nope, no press for Ms. B. hermsii… Take pity on her (or if not her, me, a hermsii survivor) and pay a visit to her fact sheet.

Poor Borrelia hermsii… No one talks about her.
If I were truly going to put my teacher hat on and plan a lesson for you, I’d tell you to make a K-W-L chart and take notes!
Once you’re done with the Borrelia sisters, you’ll probably be hungering (or worrying?) for more TBID info. Here’s a list of what’s to come: Anaplasmosis, Babesiosis (WA-1), Ehrlichiosis, Rickettsia (Rocky Mountain Spotted Fever), and more!
